Case of the Month ...

Clinical History:
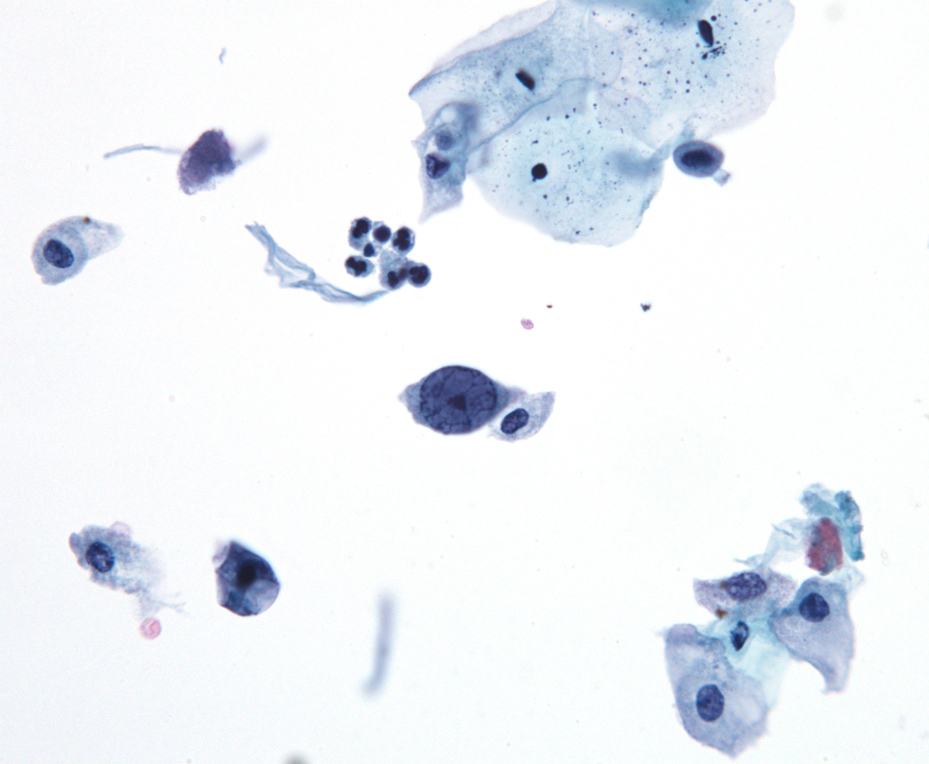
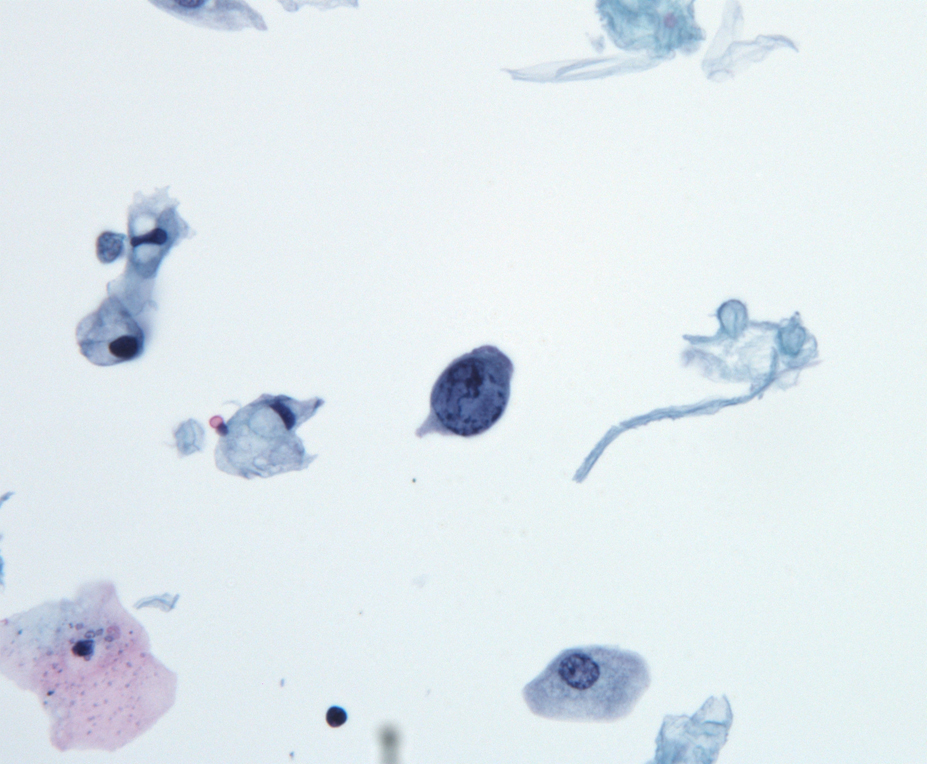
The patient is a 71-year-old man with a history of prostate cancer (pT2c) and high grade (T1a) urothelial cancer of the bladder. He is status post TURBT (transurethral resection of bladder tumor) and radical prostatectomy in 2007. Currently, his PSA is 0.05 ng/mL and has been stable over the past year. Regular follow-up urine cytology samples since 2007 have not shown recurrent urothelial cancer. He is seen in Urology clinic for routine follow up. He denies voiding dysfunction or gross hematuria. Selected images from a voided urine specimen are shown below.
Diagnosis & Discussion
click on image for larger version
Images 1-3:
ThinPrep; Papanicolaou stain, 400x magnificationQuestions:
What is the most likely cytologic diagnosis?
a. Non-specific inflammatory changes
b. High grade urothelial carcinoma
c. Prostatic adenocarcinoma
d. BK viral cytopathic effect
e. Degenerated specimen, no malignancyAll of the following are possible morphologic features of this entity except:
a. Finely granular nuclear inclusions lacking a halo
b. Large nuclei with irregular nuclear contours
c. Nucleus with an amorphous basophilic ground glass appearance
d. Large nuclei with clumped irregular chromatin
e. An eosinophilic nuclear inclusion, surrounded by a clear haloThis entity most commonly causes disease in which of the following groups of people:
a. People with a >20 pack year smoking history
b. People with systemic lupus erythematosus
c. Those of South American descent
d. People with vesicoureteral reflux
e. Renal transplant recipientsWhat is the most appropriate next step in the management of this patient?
a. Follow-up voided urine cytology in 4-6 months
b. Renal ultrasound
c. Administer a single oral dose of praziquantel
d. Cystoscopy and transurethral resection of bladder tumor (TURBT)
e. CT scan of the pelvisDiscussion:
Human polyoma viruses (BK and JC) are double-stranded DNA viruses belonging to the papovavirus family. The virus is usually acquired silently during childhood, whereafter latent infection persists for life. Up to 90% of adults are seropositive for antibodies directed against polyoma virus. Viral reactivation is not uncommon and can occur in the setting of slight changes in the immune status, usually leading to transient, asymptomatic, and self-limiting viral shedding, especially in the urothelium. Polyoma virus cellular changes are reported in 4% to 6% of urine specimens. 1
Polyoma (BK) virus-infected cells in urine cytology specimens are known to exhibit nuclear changes that mimic those of urothelial cancer. Urothelial cells with polyoma viropathic changes have been called decoy cells to warn against overdiagnosis as carcinoma. 2 Despite this, polyoma virus infected cells continue to be a relatively common cause of diagnostic error in urine cytology. 3 Four morphologic variants of nuclear inclusion bodies have been described: 1) nucleus with an amorphous basophilic ground glass appearance (most frequent); 2) an eosinophilic nuclear inclusion, surrounded by a clear halo (cytomegalovirus-like); 3) finely granular nuclear inclusions lacking a halo, and 4) large nuclei with clumped irregular chromatin (vesicular variant). 4
Although reactivation of polyoma (BK) virus is usually of no clinical consequence, there are certain populations of patients in which it has been associated with disease. Human BK virus nephropathy (BKVN) has become an important problem in renal transplantation with the use of more powerful immunosuppressive strategies. BKVN currently affects 1% to 5% of renal transplant recipients and may lead to graft failure in 45% of affected patients. 5 Urine cytology is important in the workup of BKVN. Although seeing decoy cells has a positive predictive value of 25% to 30% of predicting BKVN, their absence has a negative predictive value of 99%. 6
The role of BK virus in urothelial neoplasia is not clear. Although there are case reports demonstrating co-expression of viral protein LTag and p53 in tumor cells, the presence of this commonly-occurring virus in tumor tissue is not proof of causality. 4,7,8,9
Answers:
1. D
2. B
3. E
4. AReferences:
- Hurault de Ligny B, Godin M, Lobbedez T, et al. Virological, epidemiological and pathogenic aspects of human poyomaviruses. Presse Med. 2003;32:656-658.
- DeMay RM. The Art and Science of Cytopathology, vol. 1: Exfoliative Cytology. Chicago: ASCP Press; 1996:394-395.
- Glatz et al. An International Telecytologic Quiz on Urinary Cytology Reveals Educational Deficits and Absence of a Commonly Used Classification System. American Journal of Clinical Pathology. 2006;126:294-301.
- Herawi et al. Polyoma Virus-Associated Cellular Changes in the Urine and Bladder Biopsy Samples, A Cytohistologic Correlation. American Journal of Surgical Pathology. 2006;Volume 30, Number 3, March 2006.
- Gardner SD, Mackenzie EF, Smith C. Prospective Study of the Human Polyomavirus BK and JC and Cytomegalovirus in Renal Transplant Recipients. Journal of Clinical Pathology. 1984; 37:578.
- Bonvoisin C, Weekers L, Xhingesse P, Grosh S, Milicevic M, Krzesinski JM. Polyomavirus in Renal Transplantation: A Hot Problem. Transplantation. Volume85, Number7S, April 15 Supplement, 2008.
- Lednicky JA, Butel JS. Polyomaviruses and human tumors: a brief review of current concepts and interpretations. Front Biosci. 1999;4:D153D164.
- Roberts ISD et al. Polyoma Virus Infection and Urothelial Carcinoma of the Bladder Following Renal Transplantation. British Journal of Cancer. 2008 99(9), 1383-1386.
- Geetha D. et al. Bladder Carcinoma in a Transplant Recipient: Evidence to Implicate the BK Human Polyomavirus as a Causal Transforming Agent. Transplantation. 2002, Vol. 73, 1933-1936, No. 12.
Contributed by:
Joseph Hatem, M.D.
Fellow, University of Pennsylvania Health SystemCindy McGrath, M.D.
Associate Professor of Pathology & Laboratory Medicine
University of Pennsylvania Health System