Case of the Month ...
Clinical History:
The patient was a 48 year old woman who presented with a pelvic mass. She underwent a TAH-BSO and ileocolectomy. Two years later she presented with hilar lymphadenopathy. She underwent endobronchial ultrasound guided fine needle aspiration of an enlarged subcarinal lymph node.
Diagnosis & Discussion
click on image for larger version
Image Figs:
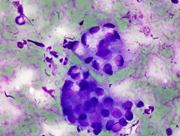
- Figure 1. FNA Direct smear, Diff-Quik stain, 100x
- Figure 2. FNA Direct smear, Pap stain, 100x
- Figure 3. FNA Direct smear, Pap stain, 100x
- Figure 4. FNA Cell block, H&E stain, 20x
Questions:
What is your diagnosis?
Metastatic adenocarcinoma with signet ring features
Clear cell RCC
Goblet cell carcinoid
High grade serous carcinoma from the ovary
What is the most common clinical presentation for the primary lesion?
Acute appendicitis
Abdominal distension and ascites
Brain and skin metastasis
Lymph node metastasis
What is thought to be the cell of origin for these lesions?
Pluripotent intestinal stem cell with disorderly differentiation
Sub epithelial neuroendocrine cells of neural crest derivation
Which one of the following is the IHC staining pattern of these lesions?
Mucin+, CK+, PAS+, chromo
Syn+, chromo+, CK-
Syn+, chromo+, PAS-
Discussion:
This woman presented with a pelvic mass. After TAH-BSO, right hemicolectomy and appendectomy, she was diagnosed with a goblet cell carcinoma (Figure 5; H&E, ovarian tumor). The tumor was widely invasive to ovaries, tubes, uterine serosa and cecum. The appendix was completely replaced by the tumor. Approximately 2 years later she presented with hilar lymphadenopathy and underwent EBUS-FNA for lymph node sampling.
The aspirate smears showed large and small clusters of epithelial cells with abundant intracytoplasmic mucin and thus low N:C ratios. Most of the nuclei were bland appearing with small nucleoli. Benign bronchial epithelial cells were the primary differential during the on-site adequacy assessment. The history of goblet cell carcinoid was crucial for making the diagnosis.
Goblet cell carcinoids, also known as appendiceal neuroendocrine tumors with mucin production, are a distinct clinical entity characterized by multidirectional differentiation. They are found almost exclusively in the appendix. Goblet cell carcinoids are a mixture of normal crypt elements, goblet cells, Paneth cells, and enterochromaffin cells. Their histologic and ultrastructural features overlap between adenocarcinoma and carcinoid tumors 2 . They are considered amphicrine tumors (endocrine and exocrine) that are thought to originate from the multipotent epithelial crypt stem cells.
Men and women are equally affected and the mean age at diagnosis is 52. The initial presentation is typically an acute appendicitis picture, often with appendiceal rupture. The clinical behavior of goblet cell carcinoids is between that of adenocarcinomas of the appendix and carcinoid tumors. The average 5 year survival rate is ~80%. Adverse prognostic features consist of serosal involvement by tumor at time of diagnosis and percentage of carcinomatous growth that is cribriform, fused glands, or singly dispersed cells, including signet ring forms. A subset of the tumors will have areas of purely adenocarcinoma differentiation which includes signet ring differentiation. These patients are more likely to present with ovarian masses, these patients have a survival that is similar to patients with conventional adenocarcinoma.
The immunohistochemical and special stain profile supports the dual differentiation. The tumor cells are positive for Pan CK, CEA, and synaptophysin. The tumor cells are negative for chromogranin, Bcl-2, p16. Useful special stains include mucicarmine and alcian blue. PAS-D staining is positive in tumors with eosinophilic granular cytoplasm.
The molecular characteristics are distinct from adenocarcinomas in that goblet cell carcinoids do not harbor k-ras mutations. Their molecular alterations are most similar to ileal carcinoids. Goblet cell carcinoids frequently contain allelic losses of 18q which is a region that contains cadherin genes, considered to be tumor suppressors.
Answer Key:
- C
- A
- A
- A
References:
• Odze, R and Goldblum, J. Surgical Pathology of the GI Tract, Liver, Biliary Tract and Pancreas: Expert Consult - Online and Print, 2e. Saunders 2009.
• Kanthan, R et al. Goblet Cell Carcinoids of the Appendix Immunophenotype and Ultrastructural Study. Archives of Pathology and Laboratory Medicine. 2001; 125: 386-390.
• Mirela, S et al. Genetic Alte rations in Goblet Cell Carcinoids of the Vermiform Appendix and Comparison with Gastrointestinal Carcinoid Tumors. Modern Pathology. 2003;16 (12):1189-1198.
Contributed by:
Jena Hudson, M.D
Cytopathology Fellow,
Washington University in St. LouisBrian T. Collins, M.D.
Section Head, Cytopathology
Washington University in St. Louis




