Case of the Month ...
Case History
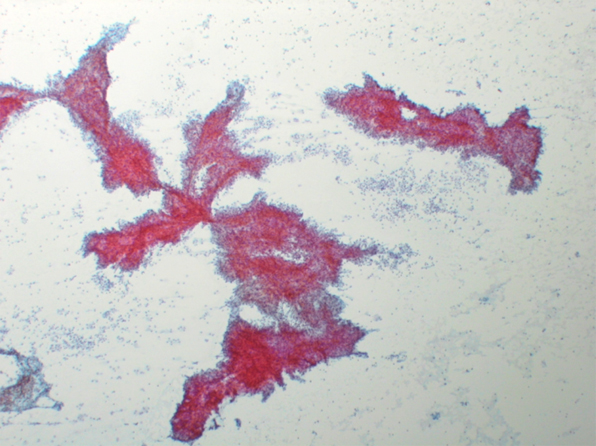
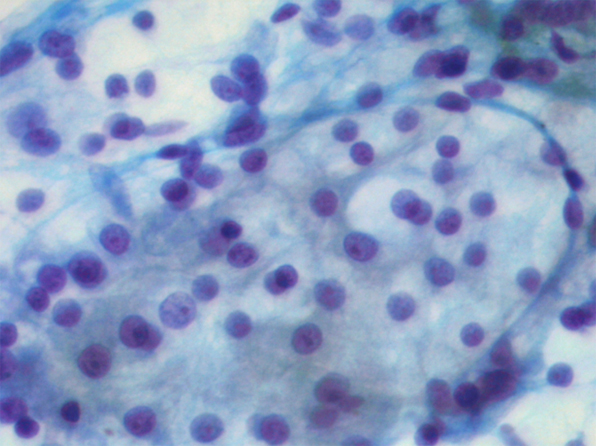
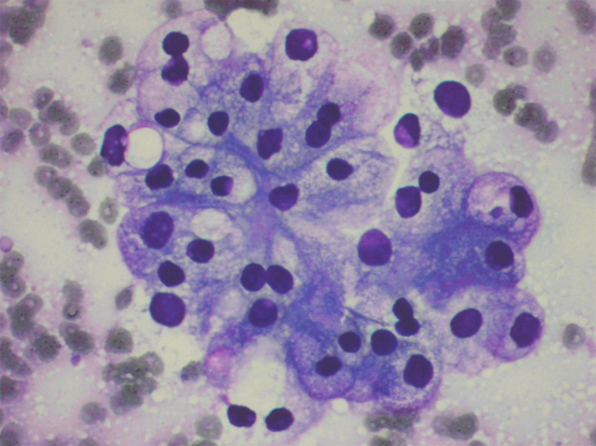
75 year old male presented with vague abdominal pain. CT scan showed multiple pancreatic nodules, ranging from 0.5 to 1.5 cm. EUS-FNA of one of the pancreatic nodules was performed. (Figure 1 to 3)
Follow Up
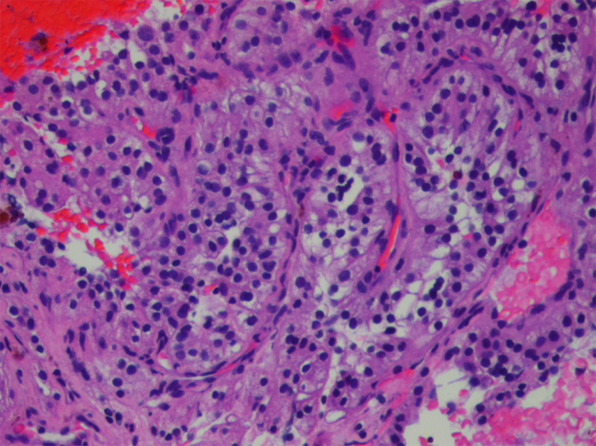
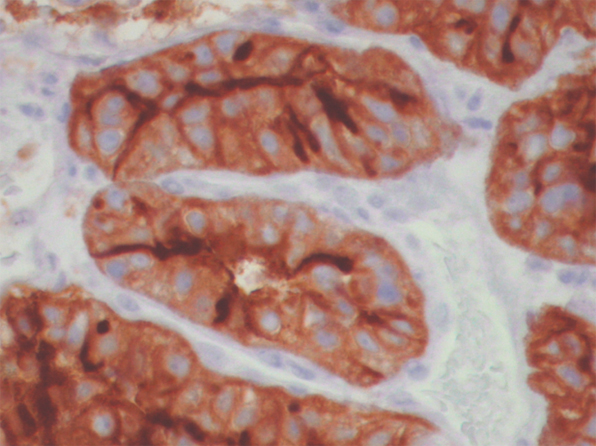
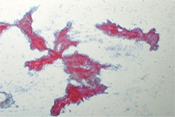
While performing on-site assessment at the endoscopy suite, the possibility of a metastatic renal cell carcinoma was raised. Upon enquiry, the patient had a renal cell carcinoma of the left kidney that was resected 5 years ago in another hospital. A cell block was prepared. (Figure 4) Immunostaining performed on the cell block showed positive staining for RCC-1, (Figure 5) CD10, cytokeratin, and vimentin.
Diagnosis & Discussion
click on image for larger version
DIAGNOSIS
Metastatic Renal Cell Carcinoma to the Pancreas
DISCUSSION
Metastases of non hematologic neoplasms to the pancreas are uncommon, accounting for 2% of all pancreatic malignancies. It can be a challenge in differentiating secondary malignancy from a primary neoplasm in the pancreas. For example, both primary and secondary malignancies present with similar symptoms including jaundice and acute pancreatitis. Both can present with a single mass and regional lymphadenopathy on imaging. The presence of a clinical history of prior malignancy should alert one about the possibility of a metastasis. However, inadequate clinical history may prevent consideration of secondary malignancies in the differential diagnosis. The presence of unusual cytologic findings such as clear cell features should raise the suspicion of metastatic disease. Additional materials should be obtained for ancillary studies such as immunohistochemistry.
Pancreatic metastases originate most commonly from lung, colon, breast, and kidney. Among these, metastases from renal cell carcinoma (RCC) deserve special attention. Metastases from renal cell carcinoma frequently occur many years after the initial resection of the primary tumor as isolated lesion. In addition, the prognosis for the patient is better than those with primary pancreatic ductal carcinoma and metastases of other origin. Therefore, it is important to correctly diagnose a metastatic RCC to the pancreas.
The typical cytologic presentation of metastatic renal cell carcinoma consists of neoplastic cells in papillary groups, irregular clusters, and singly. Individual neoplastic cells are large with relatively low nuclear/cytoplasmic ratio. The cytoplasm is abundant, and vacuolated. In a modified Giemsa (Diff-Quik) stain, the cells are characterized by numerous fine vacuoles that are sharply outlined by the intervening faintly stained cytoplasm, resulting in a clear appearance. The cytoplasm can also appear granular. Depending on the grade of the tumor, the nuclei range from small, uniform, and bland, to large and bizarre; the nuclear membranes can vary from smooth to irregular; the chromatin from fine to coarse; the nucleoli from inconspicuous to enormous. However, nuclei typically appear round to oval, relatively uniform, with fine granular chromatin and a single, prominent nucleolus. Many naked nuclei may be present.
The differential diagnosis includes other metastatic clear cell neoplasms such as hepatocellular carcinoma, adrenocortical carcinoma, and ovarian carcinoma. The use of immunohistochemistry is helpful in the differential diagnosis. RCC stains positive for CD10 and renal cell carcinoma marker (RCC-1) whereas hepatocellular carcinoma is positive for Hep1, adenocortical carcinoma for inhibin and MART1, and ovarian carcinoma for CA125. Rarely, primary pancreatic neoplasm such as islet cell tumor, acinic cell carcinoma, and well-differentiated ductal carcinoma may demonstrate clear cell features.
ACKNOWLEDGEMENT
This case is contributed by Dr. David Chhieng from the Department of Pathology, University of Alabama , Birmingham AL.