Case of the Month ...
Case History
A 48 year-old female presented with a breast mass detected on a routine mammogram. A computerized tomography displayed a 1.7 cm right breast mass abutting the chest wall with associated right axillary adenopathy. In the work-up of the breast mass, an abdominal ultrasound exam showed the presence of gallbladder polyps and multiple liver nodules. The multiple hepatic masses measured up to 2.8 cm and were radiologically suggestive of metastatic disease.
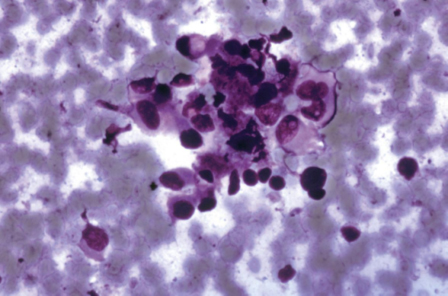
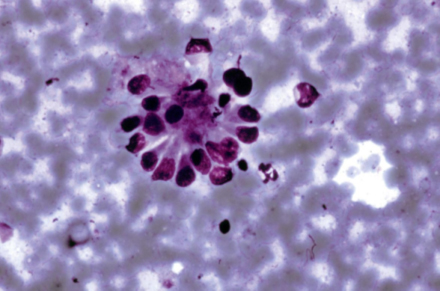
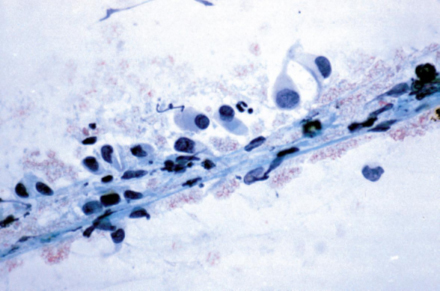
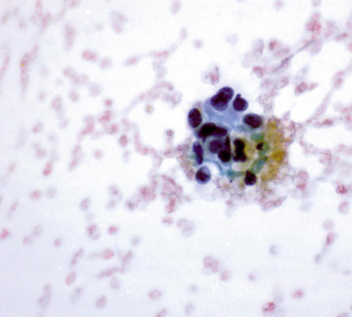
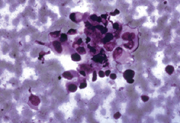
A PET scan demonstrated abnormal uptake in multiple liver lesions. A FNA of the breast mass was consistent with fibroadenoma. A CT guided FNA was performed and showed the presence of polygonal cells arranged singly as well as in small clusters. (Figure 1) Some of the clusters had a rosette or florette-like appearance. (Figure 2) The polygonal cells had dense cytoplasm with occasional vacuolization. The nuclei were eccentric resulting in a plasmacytoid appearance. (Figure 3) The chromatin was granular with inconspicuous nucleoli. Immunocytochemical studies revealed focal immunoreactivity for CK7 and CK19 (Figure 4).
Diagnosis & Discussion
click on image for larger version
Diagnosis: Hepatic epithelioid hemangioendothelioma
Discussion: Hemangioendotheliomas are vascular neoplasms of low malignant potential, which can recur and metastasize. They occur more frequently in the adulthood and are more common in women. They can involve soft tissue, bone, skin, liver, lymph node and/or lung and, not infrequently, mutifocal. Extrahepatic metastases in liver lesions occur in 28% of the cases with a mortality rate of 35%. The proposed treatment is chemotherapy or liver transplant with a 5-year survival of approximately 76%.
Histologically, there are four recognized types of hemangioendothelioma: epithelioid hemangioendothelioma, spindle cell hemangioendothelioma, kaposiform hemangioendothelioma and malignant endovascular papillary angioendothelioma. Hemangioendotheliomas, in general, are vascular neoplasms with a histological appearance intermediate between a benign hemangioma and angiosarcoma. Morphologically, they are either more atypical or more cellular than haemangioma, but they do not display the pleomorphism seen in angiosarcomas.
Despite different morphologies, all hemangioendotheliomas share the same immunohistochemical profile with immunoreactivity for CD31, CD34 and FVIII-RA. The epithelioid appearance of epithelioid hemangioendothelioma represents a potential pitfall. The main differential diagnosis of epithelioid hemangioendotheliomas is adenocarcinoma due to the epithelioid appearance and pseudo-acinar formations seen in these lesions. Features suggesting a diagnosis of hemangioendothelioma over carcinoma include hemorrhagic background and presence of angioformative structures. These structures might be wrongly interpreted as glandular differentiation. The differences are quite subtle to discern and immunocytochemical studies must be employed before a definitive diagnosis is made, but should be carefully interpreted. Cytokeratin antibodies may be misleading if not used in conjunction with vascular markers, because both epithelioid hemangioendotheliomas and carcinomas may show immunoreactivity for cytokeratin. Epithelioid vascular neoplasms may be immunoreactive for epithelial markers including keratin, B72.3, and EMA. However, only epithelioid vascular neoplasms, including hemangioendotheliomas, are immunoreactive for vascular markers (CD31, CD34, UEA, and FVIII-RA) as opposed to carcinomas, which are not immunoreactive.
Surgical follow up
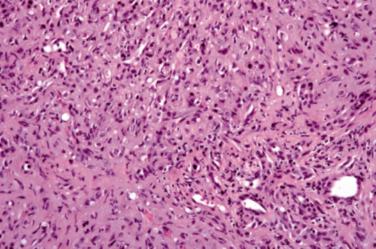
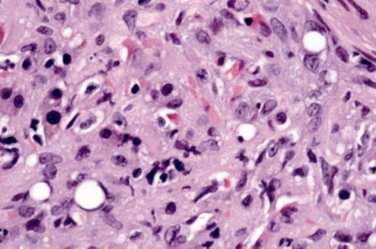
The FNA was followed by an open surgical biopsy. Histology was consistent with an epithelioid hemangioma. (Figure 5 and 6)
Acknowledgement:
This case is submitted by Oscar Lin MD from the Department of Pathology, Memorial Sloan Kettering Cancer Center , New York , NY