Case of the Month ...
Case History
The patient is a 64 year old African-American woman with history of metaplastic carcinoma of right breast; S/P partial mastectomy and right axillary dissection (T2,N0) in 1992. She was treated post-operatively with chemo- and radiation therapy. In March 2001, she underwent bilateral mastectomy followed by chemotherapy. In June 2001, she presented with a 3 cm fluctuating nodule in mid-chest. FNA of this nodule yielded drops of old blood with only partial collapse of the nodule. Two weeks later, an excisional biopsy of the nodule was performed.
To discuss this case with your colleagues, join the PSCO mailing list
Diagnosis & Discussion
click on image for larger version
MICROSCOPIC DESCRIPTION
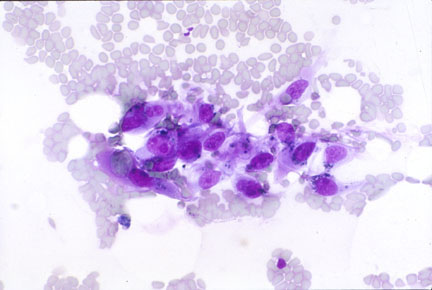
Cytologic Image 1: Hypocellular smear with scattered primarily single, noncohesive, large, plump spindled cells. The nucleus is eccentric, pleomorphic and with prominent nucleolus. The cytoplasm is abundant, tapers into the background, pale and finely vacuolated.
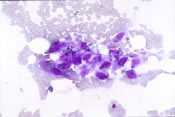
Cytologic Image 2: Occasional cluster of 5-10 cells showing similar cytologic features as in image 1. Few of these cells contain cytoplasmic hemosiderin.
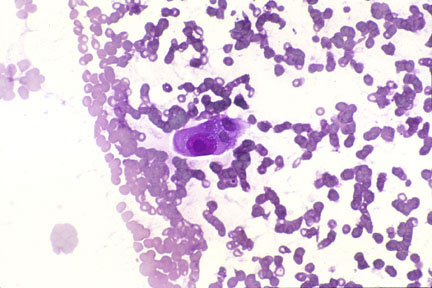
Cytologic Image 3: Hypocellular smear showing a single atypical cell with mitosis in a background of blood.
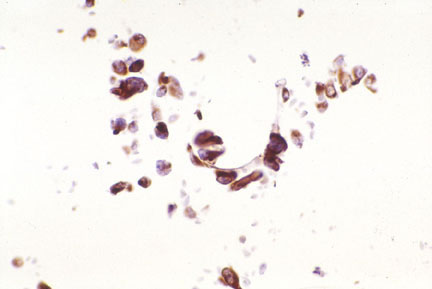
Cytologic Image 4: The tumor cells show immunoreactivity to CD31.
FNA DIAGNOSIS
Angiosarcoma
HISTOLOGIC FINDINGS
- Surgical 1: High grade angiosarcoma showing almost solid areas of tumor composed of pleomorphic cells with an attempt at vascular channel formation. The tumor also shows hemorrhagic areas.
- Surgical 2: Higher magnification showing a vascular channel lined by plump, pleomorphic tumor cells showing the cytologic features identical to those seen in the needle aspirate preparations. Note the high mitotic activity.
HISTOLOGIC DIAGNOSIS
Angiosarcoma
DISCUSSION
Angiosarcomas are collectively one of the rarest forms of soft tissue neoplasms and account for less than 1% of all sarcomas. The presentation and behaviour of these tumors differ depending on location, and any predisposing conditions. Hence they are more appropriately considered as several closely related tumors rather than as a single entity. Enzinger and Weiss have divided them into five groups:
- Cutaneous angiosarcoma unassociated with lymphedema;
- Cutaneous angiosarcoma associated with lymphedema;
- Angiosarcoma of the breast;
- Radiation-induced angiosarcoma; and
- Angiosarcoma of deep soft tissue.
Angiosarcomas of the breast arise spontaneously exclusively in women, usually during the third or fourth decade, or as a complication of radiation therapy after breast conserving surgery. There is a 0.3% to 4% risk of angiosarcoma after radiation therapy for breast cancer, with most cases arising 5 to 10 years after treatment. Angiosarcomas can also arise in the skin of a chronically edematous arm after mastectomy (Stewart-Treves syndrome), but this complication has become much less common with greater attention to surgical techniques.
The FNA is hemorrhagic and usually hypocellular. Cytologically depending upon the grade of the tumor, the cells can be bland (resembling a hemangioma) to bizarre spindled cells with eccentric, pleomorphic nuclei showing prominent nucleoli. The cytoplasm is abundant and may contain distinct vacuoles containing fragmented red blood cells or their by-products. Primitive vascular structures in the form of microacini or pseudopapillary clusters can be seen. Necrosis may be seen in high grade tumors.
The differential diagnosis includes hemangioma, angiolipoma and granulation tissue, particularly in low grade tumors.
This case fits the classic example of post-radiation angiosarcoma occuring 9 years after breast conserving surgery and radiation therapy. Lymphedema of the arm was never a post-operative complication in this case.